PCOS Androgen Excess: Fertility Solutions
Struggling with PCOS and fertility? Here's what you need to know: High androgen levels in PCOS can disrupt ovulation, making conception difficult. This hormonal imbalance affects millions of women in the U.S., leading to irregular cycles, anovulation, and symptoms like acne or unwanted hair growth. The good news? There are effective solutions.
Key takeaways:
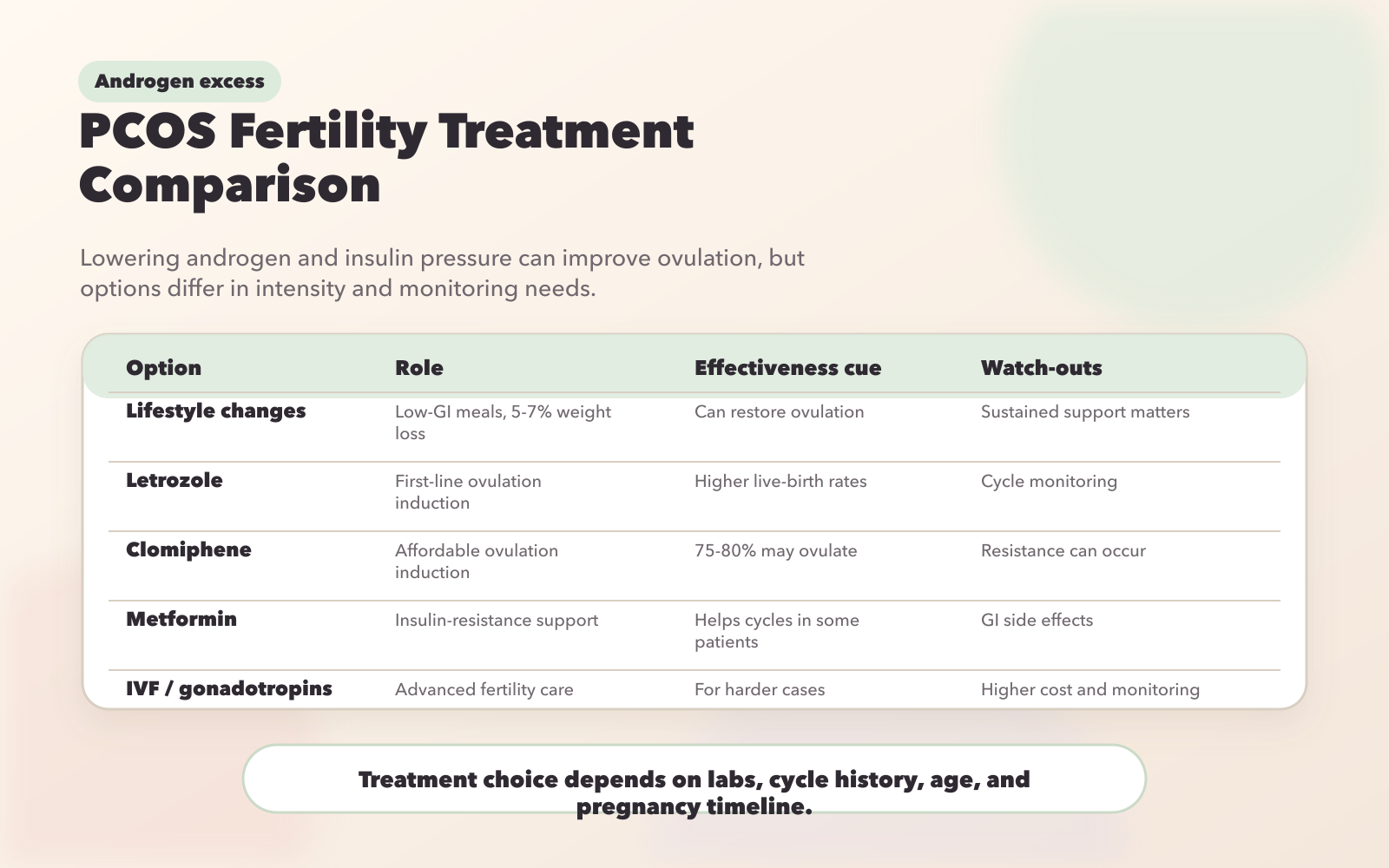
- Lifestyle changes: Losing 5–7% of body weight can restore ovulation and reduce androgens.
- Diet tips: Focus on low-GI foods, stabilize blood sugar, and consider supplements like inositol or Vitamin D.
- Exercise: Regular physical activity, especially HIIT, improves insulin sensitivity and hormonal balance.
- Medical treatments: First-line options like letrozole (27.5% live birth rate) and clomiphene citrate can induce ovulation. Metformin helps if insulin resistance is present.
- Advanced options: Gonadotropins and IVF are available for more challenging cases.
Understanding your body and working with a healthcare provider can help you navigate PCOS-related fertility challenges. Whether through lifestyle adjustments, medications, or advanced treatments, tailored approaches can improve your chances of conceiving.
PCOS and Fertility: What Treatment Actually Works (Backed by Science)
How High Androgen Levels Affect Fertility in PCOS
High levels of androgens disrupt critical reproductive functions, making it harder to conceive. These hormones interfere with the precise hormonal signals needed to release a mature egg each month .
Ovulation Disruption
Excess androgens accelerate GnRH pulses, throwing off the balance between luteinizing hormone (LH) and follicle-stimulating hormone (FSH). This imbalance leads the pituitary gland to produce too much LH and not enough FSH - an essential hormone for egg maturation.
"Excess androgen suppresses the expression of cumulus expansion-related genes and oocyte maturation-related genes, causing excess small growing follicles to be arrested at the antral stage, inhibiting the development of the dominant follicle." – Wang et al., Frontiers in Endocrinology
Because of this, the ovaries develop multiple small follicles that remain stuck in an early stage rather than maturing into a dominant follicle needed for ovulation. Additionally, elevated levels of dihydrotestosterone (DHT) increase Anti-Müllerian hormone (AMH) levels - often 2 to 3 times higher than in women without PCOS - making the follicles less responsive to FSH. On a cellular level, high androgen levels cause oxidative stress and mitochondrial dysfunction in granulosa cells, leading to cell death and reducing both the number and quality of eggs available for fertilization.
These ovulation issues are further complicated by insulin resistance.
Insulin Resistance and Fertility
Insulin resistance and excess androgens create a harmful cycle that worsens fertility problems. About 75% of women with PCOS experience insulin resistance, which drives additional androgen production. Elevated insulin levels stimulate ovarian cells to produce more androgens through the CYP17 pathway .
High insulin also reduces the liver's production of sex hormone-binding globulin (SHBG), increasing levels of free, active testosterone. This amplifies androgen-related effects and sets off a feedback loop: excess androgens encourage abdominal fat storage, which worsens insulin resistance and leads to even more androgen production .
"Insulin resistance and the compensatory hyperinsulinemia are central mechanisms that perpetuate anovulation and lead to metabolic complications." – Ana L Rocha, Department of Obstetrics and Gynecology, Universidade Federal de Minas Gerais
Excess androgens also cause oxidative stress, which harms oocyte quality and embryo development . Breaking this cycle through lifestyle adjustments - such as losing just 5% to 7% of body weight - can lower insulin and androgen levels, often restoring spontaneous ovulation in many women. Combining targeted lifestyle changes with hormonal treatments can significantly improve fertility outcomes.
Lifestyle Changes to Lower Androgens and Improve Fertility
Certain lifestyle adjustments can help lower androgen levels and restore ovulation by breaking the insulin–androgen cycle often seen in PCOS.
Weight Loss
Shedding just 5% of body weight can significantly improve SHBG production, restore ovulation, and enhance insulin sensitivity. It also reduces levels of androstenedione and luteinizing hormone (LH), helping to correct the hormonal imbalance that disrupts follicle development. At the same time, it decreases inflammation markers like C-reactive protein (CRP). A combination of cutting 500–1,000 calories daily and incorporating regular exercise is often enough to trigger ovulation.
"If a woman is overweight and has polycystic ovaries, the most helpful thing that she can do is exercise and achieve weight loss." – Stephen Greenhouse, M.D., Shady Grove Fertility
Dietary changes can further support weight loss and regulate insulin and androgen levels.
Diet Modifications
Diet plays a direct role in controlling insulin production, which is a key factor in excess androgen production. A low-glycemic index (GI) diet helps stabilize blood sugar levels, reducing the need for insulin and signaling the ovaries to produce less testosterone, ultimately improving fertility outcomes.
To maintain stable blood sugar, replace high-GI foods with options like whole grains, lean proteins, and non-starchy vegetables. Steer clear of sodas, fruit juices, and foods high in added sugars, as these can cause rapid insulin spikes. Additionally, evidence suggests that supplementing with inositol - specifically in a 40:1 ratio of myo-inositol to D-chiro-inositol - may lower testosterone levels and promote ovulation. Addressing Vitamin D deficiency is also important, as nearly 75% of women with PCOS have levels below 30 ng/mL, which can impact both fertility and glucose tolerance.
Beyond diet, exercise is a key factor in restoring hormonal balance and reducing stress.
Exercise and Stress Reduction
Regular physical activity can lower insulin resistance and support ovulation. High-intensity interval training (HIIT) is particularly effective at reducing body fat and insulin resistance, while resistance training helps build muscle and improves glucose metabolism. Aim for at least 150 minutes of exercise each week, as every hour of vigorous activity lowers the risk of metabolic syndrome by 22%.
"With weight loss and exercise, some women end up ovulating regularly on their own, or they respond better to fertility medications." – Stephen Greenhouse, M.D., Shady Grove Fertility
Stress management is equally important, as women with PCOS are more likely to experience depression and anxiety - conditions that can disrupt hormones and make it harder to stick with lifestyle changes. Joining peer support groups can ease psychological stress and reinforce healthy habits. Plus, exercise releases irisin, a compound that may help reduce anxiety while boosting metabolism.
Hormonal Therapy Options for PCOS Fertility
Once lifestyle changes have been implemented, hormonal therapies can provide an additional layer of support for women with PCOS who are trying to conceive. These treatments are designed to address hormonal imbalances, either by encouraging the ovaries to release eggs or by reducing high androgen levels that disrupt normal ovulation. By directly targeting the hormonal disruptions caused by PCOS, these therapies work hand-in-hand with lifestyle adjustments to improve fertility outcomes.
Letrozole for Ovulation Induction
Letrozole has become the go-to option for ovulation induction in women with PCOS. This medication, originally developed as a breast cancer treatment, works by blocking estrogen production, which in turn stimulates ovulation. Studies show that letrozole achieves a live birth rate of 27.5%, outperforming clomiphene citrate, which has a rate of 19.1%.
"The aromatase inhibitor letrozole seems to be more effective than the reference drug clomiphene citrate to treat infertility due to PCOS." – Ana L. Rocha, Department of Obstetrics and Gynecology, Universidade Federal de Minas Gerais
Letrozole’s off-label use for fertility has now become a standard approach, offering many women a better chance at achieving pregnancy.
Clomiphene Citrate and Metformin Combination
Clomiphene citrate, often referred to as Clomid, is another widely used medication for inducing ovulation. It works by modulating estrogen receptors, which prompts the body to produce more follicle-stimulating hormone (FSH) and luteinizing hormone (LH), both of which are essential for ovulation. However, not all women respond to clomiphene alone - this is known as clomiphene resistance.
For women experiencing clomiphene resistance, combining it with metformin can be a game-changer. Metformin improves insulin sensitivity and reduces hyperinsulinemia, which helps lower excessive androgen production by the ovaries. This combination has been shown to boost both ovulation rates and clinical pregnancy success.
Spironolactone and Anti-Androgen Treatments
Spironolactone is a medication that blocks androgen receptors and reduces circulating androgen levels, making it highly effective for managing symptoms like acne and unwanted facial hair. While it doesn’t directly promote ovulation, spironolactone can help control androgen-related issues before active fertility treatments begin.
Important safety reminder: Spironolactone should be discontinued before attempting pregnancy due to the risk it poses to a male fetus, such as feminization. Women taking spironolactone should use reliable contraception until they are ready to transition to ovulation-inducing therapies like letrozole.
For those managing androgen-related symptoms, services like Oana Health offer spironolactone through telehealth consultations. Women can access personalized care from licensed professionals and receive treatments conveniently delivered to their homes with free shipping.
sbb-itb-6dba428
Advanced Fertility Treatments for PCOS
When medications like letrozole or clomiphene don’t lead to successful conception, advanced fertility treatments become the next step. These methods specifically address the challenges posed by hormonal imbalances and androgen excess in PCOS. While they require close medical supervision, they offer additional opportunities for women struggling with fertility issues.
Gonadotropins for Ovulation Stimulation
Gonadotropins, which are injectable forms of follicle-stimulating hormone (FSH) or human menopausal gonadotropin (hMG), directly encourage the ovaries to develop follicles. Typically, treatment begins with daily injections on cycle days 3–5. Once the follicles reach a size of 16–18 mm, an injection of human chorionic gonadotropin (hCG) is administered to trigger ovulation.
For women with PCOS, many clinicians recommend the chronic low-dose protocol, starting with doses of 37.5–75 IU and gradually increasing as needed. This cautious approach lowers the risk of ovarian hyperstimulation syndrome (OHSS) and reduces the likelihood of multiple pregnancies, while still achieving effective results. Research indicates that gonadotropin therapy can produce cumulative pregnancy rates of about 90%, with cumulative live birth rates reaching 85% after 12 cycles. However, the risk of miscarriage remains slightly higher at 20–25%, compared to a background rate of 15%. Regular monitoring with ultrasounds and blood tests ensures that only one or two follicles mature, minimizing complications.
If ovarian stimulation alone doesn’t lead to success, in vitro fertilization (IVF) becomes a viable next step, offering a more controlled and laboratory-assisted approach.
IVF and Managing OHSS Risks
In vitro fertilization (IVF) is often considered when ovulation induction isn’t effective or when additional infertility factors, such as blocked fallopian tubes or male infertility, are involved. During IVF, eggs are retrieved from the ovaries, fertilized in a lab, and then transferred back into the uterus as embryos.
Women with PCOS tend to have a higher number of antral follicles - 12 to 20 or more per ovary - which increases their risk of developing OHSS during IVF. To address this, fertility specialists often include GnRH antagonists in the IVF protocol. These medications help control the ovarian response by suppressing the release of luteinizing hormone (LH) and FSH from the pituitary gland, allowing for safer options when triggering ovulation.
Before starting IVF, it’s essential to rule out other potential causes of infertility and ensure overall health is optimized. For example, screening for conditions like obstructive sleep apnea, which is more common in women with PCOS, is an important part of preparation.
Treatment Comparison for Androgen Excess and PCOS Fertility
PCOS Fertility Treatment Comparison: Effectiveness and Side Effects
Understanding the hormonal imbalances associated with androgen excess and PCOS is key to selecting the right treatment. Your choice of therapy should align with your fertility goals, body mass index (BMI), and insulin resistance. Each treatment option comes with its own advantages and potential side effects, which are summarized below.
Hormonal Therapy Comparison Table
| Therapy | Effectiveness for Fertility | Notable Side Effects | Best Suited For | Important Considerations |
|---|---|---|---|---|
| Letrozole | 27.5% live birth rate; 61.7% ovulation rate | Generally well tolerated; minimal antiestrogen effects | First-line for ovulation induction, especially in patients with higher BMI | Short half-life (~45 hours) helps maintain endometrial receptivity |
| Clomiphene Citrate | 19.2% live birth rate; 22% pregnancy rate per cycle | Hot flashes, mood swings; 8–13% risk of multiple pregnancies | Traditional first-line treatment for anovulatory PCOS | Longer half-life may thin the uterine lining |
| Metformin | Limited effectiveness as monotherapy; improves outcomes when combined with clomiphene | Gastrointestinal issues like bloating, diarrhea, and nausea | Patients with insulin resistance or glucose intolerance | Start with 500 mg and increase gradually, taking with food to reduce side effects |
| Gonadotropins | ~70% monofollicular ovulation rate | Risk of ovarian hyperstimulation syndrome and ~5.7% rate of multiple pregnancies | Second-line option when oral agents fail | Requires close monitoring with ultrasounds and blood tests |
| Spironolactone | Not suitable during conception attempts | Dizziness, hyperkalemia, low blood pressure | Managing hirsutism and acne | Discontinue at least 3 months before trying to conceive |
This table provides a snapshot of each therapy's role in treating PCOS-related fertility challenges. Below, we dive deeper into the specifics of these treatments.
For instance, the PPCOS II trial revealed that letrozole achieved a live birth rate of 27.5%, outperforming clomiphene citrate (CC), which had a rate of 19.2%. Dr. Ana L. Rocha from Universidade Federal de Minas Gerais highlights this difference:
"The major advantage of letrozole over CC is better ovulation-inducing response, especially in obese patients, which translates into higher pregnancy and live birth rates"
In cases where clomiphene resistance is an issue, combining metformin with clomiphene can lead to improved outcomes for insulin-resistant patients. However, it’s critical to note that spironolactone, often used to manage hirsutism, must be stopped at least three months before attempting to conceive. For those managing symptoms like hirsutism while postponing pregnancy, spironolactone can be paired with contraception, often through services like Oana Health's telehealth platform.
When oral medications fail to deliver results, gonadotropins are a valuable second-line option. These treatments, however, demand close monitoring due to the heightened risk of ovarian hyperstimulation syndrome and multiple pregnancies. Low-dose protocols aim for a monofollicular ovulation rate of about 70%, with a multiple pregnancy rate of approximately 5.7%.
Each treatment option offers different pathways to address fertility challenges in PCOS, making informed decision-making essential.
Conclusion
Effectively managing androgen excess in PCOS requires a personalized approach that targets both fertility and long-term metabolic health. Even small lifestyle adjustments, like achieving a modest 5% weight loss, can help restore ovulation. On the medical front, treatments like letrozole have shown promising results, with live birth rates reaching 27.5%. Collaborating with healthcare professionals ensures your treatment plan aligns with your unique reproductive goals.
"The therapeutic plan should be tailored to the patient phenotype, complaints, and reproductive desire." – Dr. Ana L. Rocha, Universidade Federal de Minas Gerais
This highlights the importance of working with specialists who understand the complexities of PCOS. Platforms such as Oana Health provide convenient access to personalized care through telehealth. They offer science-supported treatments for insulin resistance, hormonal imbalances, and fertility challenges - all delivered right to your doorstep.
From lifestyle modifications to advanced medical therapies, every step in managing PCOS is aimed at restoring hormonal balance. Whether you're considering medications like metformin or exploring advanced fertility options, professional guidance is key. A tailored approach - ranging from achieving a small weight reduction to using therapies like letrozole - can significantly improve ovulation and fertility outcomes.
"Integral management by a multidisciplinary team may help the patients to adhere to lifestyle interventions and thereby reduce body adiposity and recover their metabolic and reproductive health." – Dr. Ana L. Rocha
With the right support, including telehealth services from Oana Health, you can create a plan that addresses both your immediate fertility goals and long-term health needs. PCOS-related fertility challenges are manageable when you have a treatment plan designed specifically for you.
FAQs
How do elevated androgen levels in PCOS impact ovulation?
Elevated androgen levels in PCOS disrupt the normal growth and function of ovarian follicles, which play a key role in ovulation. This hormonal imbalance often leads to chronic anovulation, meaning ovulation happens irregularly or not at all.
On top of that, excessive androgens can reduce the production of progesterone - an essential hormone for maintaining regular menstrual cycles and supporting reproductive health. By managing androgen levels with specific treatments, it’s possible to rebalance hormones and promote healthier ovulation.
What lifestyle changes can help manage androgen levels and improve fertility in women with PCOS?
Lifestyle adjustments targeting insulin resistance and promoting healthy weight management can play a big role in reducing androgen levels and improving fertility for women with PCOS. A low-glycemic, balanced diet - featuring whole grains, legumes, non-starchy vegetables, lean proteins, and healthy fats - can help stabilize blood sugar, enhance insulin sensitivity, and decrease ovarian testosterone production.
Staying active is just as important. Try to get at least 150 minutes of moderate aerobic exercise or 75 minutes of vigorous activity each week. Pairing regular exercise with a modest reduction in calorie intake can lead to a 5–10% weight loss, which has been shown to lower free androgen levels and improve ovulation. Adding strength training to your routine can further improve insulin sensitivity by building muscle.
Other lifestyle factors matter too. Aim for 7–9 hours of quality sleep each night, explore stress management techniques like yoga or mindfulness, and steer clear of smoking or excessive alcohol use. For those who want extra support, Oana Health provides personalized telehealth programs that combine lifestyle coaching with evidence-based hormonal treatments, all from the comfort of your home.
What’s the difference between letrozole and clomiphene citrate for ovulation induction in women with PCOS?
Letrozole and clomiphene citrate are two medications commonly used to help women with PCOS (polycystic ovary syndrome) ovulate, but they work in different ways and come with their own benefits. Clomiphene citrate, a selective estrogen receptor modulator (SERM), stimulates ovulation by blocking estrogen receptors in the brain. This blockage prompts the brain to produce more hormones that trigger ovulation. However, clomiphene can sometimes lead to unwanted effects, such as thinning the uterine lining or altering cervical mucus, which may cause "clomiphene resistance" in some women.
On the other hand, letrozole, an aromatase inhibitor, works by reducing estrogen production. This approach avoids the side effects associated with clomiphene, making it a suitable alternative for women who don’t respond to clomiphene or experience its drawbacks.
Research suggests letrozole often leads to better outcomes. For instance, a large study found live birth rates of 27.5% with letrozole compared to 19.1% with clomiphene. Letrozole is also less likely to cause complications such as ovarian hyperstimulation syndrome or multiple pregnancies. In terms of dosing, clomiphene is typically prescribed at 50–150 mg daily for five days, while letrozole is usually given at 2.5–7.5 mg daily for the same duration.
For women seeking personalized fertility treatments, Oana Health offers telehealth services that include prescription-based options like letrozole and clomiphene. Their licensed medical professionals work with you to design a tailored treatment plan, which is then conveniently delivered to your doorstep.