PCOS Hair Loss vs. Menopause Hair Loss
Hair loss in women often stems from hormonal changes, but the causes and patterns differ significantly between PCOS and menopause. Here's what you need to know:
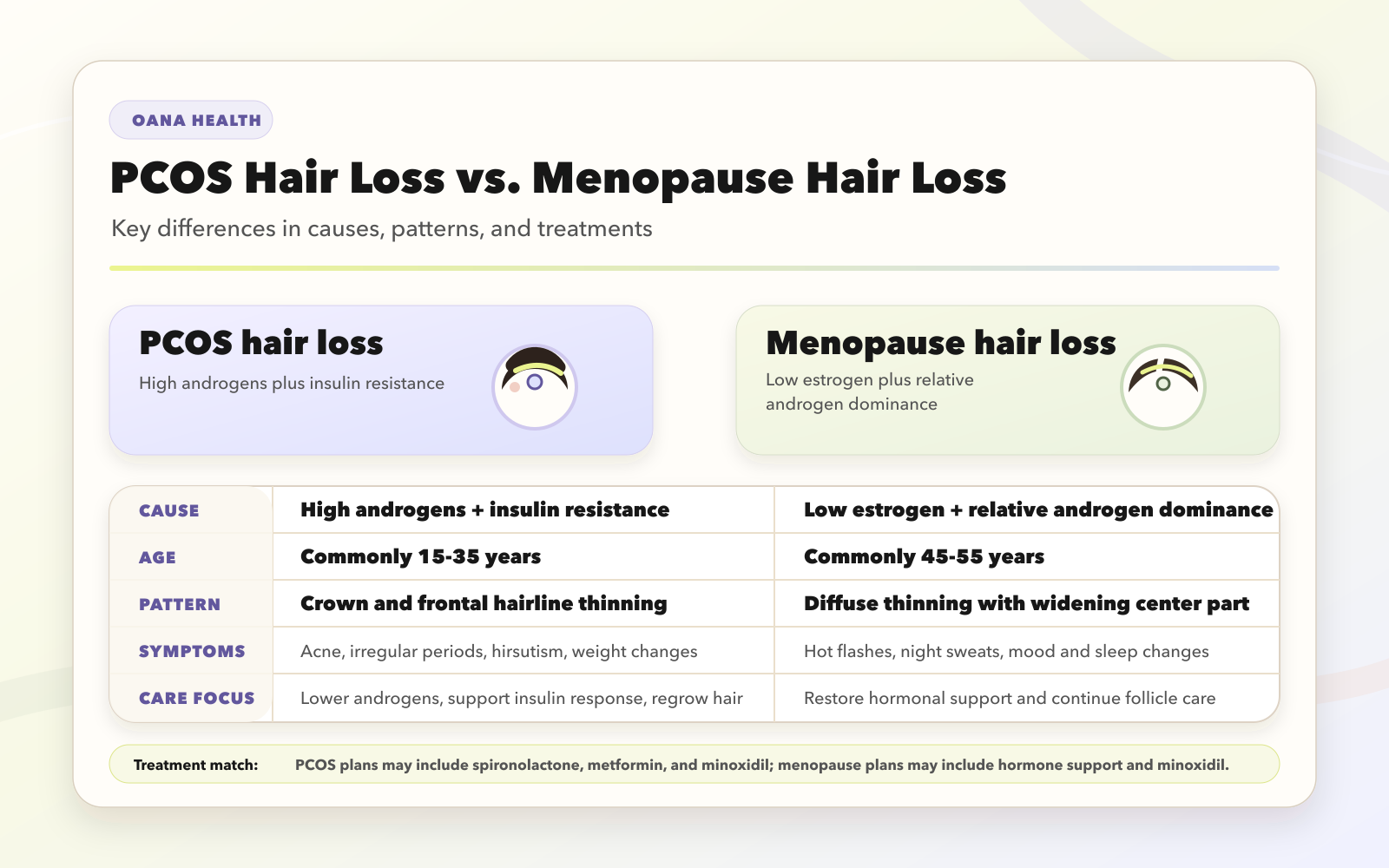
- PCOS Hair Loss: Triggered by high androgen levels and insulin resistance, it typically starts in adolescence or early adulthood. Hair thins around the crown and frontal hairline, resembling male-pattern baldness. Symptoms may include acne, irregular periods, and hirsutism (excess hair growth on the body).
- Menopause Hair Loss: Caused by declining estrogen and progesterone levels, leading to relative androgen dominance. It usually begins after age 40, with diffuse thinning across the scalp (especially the top and center), while the frontal hairline remains intact. Symptoms often include hot flashes and mood changes.
Quick Comparison
| Feature | PCOS Hair Loss | Menopause Hair Loss |
|---|---|---|
| Cause | High androgens, insulin resistance | Low estrogen, relative androgen dominance |
| Age Range | 15–35 years | 45–55 years |
| Hair Pattern | Crown, frontal hairline thinning | Diffuse thinning, widening center part |
| Reversibility | Often reversible with early treatment | Requires continuous management |
| Key Treatments | Spironolactone, Metformin, Minoxidil | Hormone Replacement Therapy, Minoxidil |
To address hair loss, treatments must target the specific hormonal imbalance. For PCOS, this means reducing androgens and managing insulin resistance. For menopause, restoring estrogen levels is key. Early intervention can improve outcomes for both conditions.
PCOS vs Menopause Hair Loss: Key Differences in Causes, Patterns, and Treatments
Hormonal Differences Between PCOS and Menopause
PCOS: High Androgens and Insulin Resistance
Hair loss in PCOS is primarily linked to elevated levels of androgens, particularly testosterone and DHT. These hormones, produced in excess by the ovaries and adrenal glands, directly harm hair follicles, causing them to shrink over time. A key characteristic of PCOS is insulin resistance, which affects about 70% of individuals with the condition.
High insulin levels play a pivotal role by encouraging the ovaries to produce more testosterone and reducing SHBG (sex hormone-binding globulin). This reduction increases free testosterone levels, which further damages hair follicles. This creates a feedback loop where elevated insulin drives up free testosterone, leading to ongoing follicle miniaturization.
"The pathophysiology of PCOS primarily involves insulin resistance and a high prevalence of visceral adiposity... which causes errors in hormonal cross-talk between the hypothalamus, pituitary gland, and ovaries." – StatPearls
While PCOS-related hair loss is tied to androgen excess and insulin resistance, menopausal hair loss follows a different hormonal pathway.
Menopause: Low Estrogen and Androgen Dominance
During menopause, hair loss occurs as estrogen and progesterone levels drop, removing their protective effects on hair follicles. Even if androgen levels remain stable or slightly decrease, the sharp decline in estrogen creates a situation of relative androgen dominance. Without sufficient estrogen, androgens bind more readily to scalp receptors, resulting in follicle shrinkage. This type of hair loss tends to be diffuse, with hair becoming finer and weaker over time.
The table below highlights the distinct hormonal mechanisms behind hair loss in PCOS and menopause.
Comparison Table: Hormonal Triggers
| Feature | PCOS Hair Loss | Menopause Hair Loss |
|---|---|---|
| Primary Hormonal Driver | Absolute androgen excess & insulin resistance | Relative androgen dominance due to low estrogen |
| Key Hormone Levels | ↑ Testosterone, ↑ DHT, ↑ Insulin, ↑ LH | ↓ Estrogen, ↓ Progesterone, ↑ FSH |
| Typical Age of Onset | 15–35 years (reproductive years) | 45–55 years (post-reproductive years) |
| SHBG Levels | Low (increases free androgens) | Generally stable |
| Associated Symptoms | Acne, hirsutism, irregular periods, weight gain | Hot flashes, night sweats, mood changes |
Hair Loss Patterns: PCOS vs. Menopause
PCOS: Crown and Frontal Hairline Thinning
Hair loss from PCOS tends to focus on the crown and frontal hairline, often leading to noticeable bald spots in more advanced stages. This pattern is similar to male-pattern baldness, affecting specific areas rather than the entire scalp. Elevated DHT levels play a major role, shrinking hair follicles, shortening the growth cycle, and weakening individual strands. Interestingly, about 70% of individuals with PCOS also experience hirsutism - excessive hair growth on areas like the face, chest, or abdomen - creating a frustrating contrast to the thinning hair on the scalp.
On the other hand, menopausal hair loss presents a more generalized thinning pattern.
Menopause: Overall Scalp Thinning
Hair loss during menopause typically appears as diffuse thinning across the entire scalp, rather than forming concentrated bald spots. This often begins with a widening center part, making the scalp more visible over time. Unlike PCOS, menopausal hair loss usually spares the frontal hairline, which is a key distinguishing factor.
"In women, the frontal hairline is typically spared with diffuse hair loss at the crown and top of the head, with loss often marked by a wider center part." – StatPearls
Roughly two-thirds of women notice significant thinning or even complete hair loss after menopause. The hair gradually becomes finer, shorter, and weaker as follicles shrink, but complete baldness is uncommon. While PCOS-related hair loss may be reversed with timely treatment, menopausal thinning tends to be permanent unless actively addressed.
These distinct patterns highlight the importance of specialized approaches to treatment.
Comparison Table: Hair Loss Patterns
| Feature | PCOS Hair Loss | Menopause Hair Loss |
|---|---|---|
| Affected Areas | Crown, temples, frontal hairline (receding) | Top of head, center part, overall scalp (diffuse) |
| Visual Pattern | Resembles male-pattern baldness; may include bald patches | Widening part line; finer, shorter hair |
| Hairline Changes | May involve receding or thinning at the front | Frontal hairline usually remains intact |
| Accompanying Hair Symptoms | Hirsutism (facial/body hair), acne | New unwanted hair growth, e.g., on the chin |
| Reversibility | Often reversible with early hormonal treatment | Typically permanent without intervention |
Treatment Options for PCOS and Menopause Hair Loss
PCOS Hair Loss: Tackling Androgens and Insulin Resistance
Addressing PCOS-related hair loss involves targeting excess androgens and insulin resistance. Oral contraceptives containing estrogen and progestin help lower androgen levels and regulate menstrual cycles. Anti-androgens like Spironolactone work by blocking testosterone's effects on hair follicles, preventing further thinning. For those with insulin resistance, Metformin enhances the body’s insulin response, which can indirectly reduce androgen production.
Topical Minoxidil (available in 2% and 5% concentrations) is another effective option. It promotes hair regrowth by extending the hair's growth phase. While initial results may appear within 3 to 6 months, full recovery typically takes 9 to 12 months. For more advanced interventions, treatments like PRP (platelet-rich plasma) and microneedling can activate dormant hair follicles.
Lifestyle changes are equally important. Modest weight loss can restore ovulation and reduce androgenic symptoms, while following a low-glycemic index diet can help stabilize insulin levels. Engaging in at least 150 minutes of moderate exercise weekly improves insulin sensitivity and lowers stress-induced cortisol levels. Some natural remedies, like spearmint tea and saw palmetto, are believed to lower free testosterone and block DHT. Together, these adjustments contribute to better hormonal balance.
For those seeking convenient care, Oana Health offers tailored telehealth treatments. Options include Spironolactone starting at $14/month, Oral Minoxidil for $25/month, and combination packs like Metformin & Spironolactone at $32/month. All prescriptions are provided by licensed professionals and shipped to your doorstep with free delivery.
Shifting focus, menopausal hair loss requires strategies centered on hormonal support and ongoing care.
Menopause Hair Loss: Supporting Hormonal Changes
When it comes to menopausal hair loss, treatments focus on restoring hormonal balance and aiding aging hair follicles. Hormone Replacement Therapy (HRT) can replenish declining estrogen levels, helping to slow hair thinning. Topical Minoxidil (2% or 5%) remains a go-to solution for promoting regrowth. Unlike PCOS-related hair loss, menopausal thinning often requires continuous management.
"Early treatment of alopecia may reduce the speed of thinning and promote regrowth." – Cleveland Clinic
Additional measures include using sulfate-free shampoos and avoiding high-heat styling tools to protect fragile hair. Maintaining a nutrient-rich diet and prioritizing adequate sleep also support a healthy hair growth cycle.
Telehealth services simplify access to dermatologists and hormone specialists, allowing for remote monitoring and adjustments to treatment plans. Oana Health offers comprehensive solutions, including hormone support and hair care, all from the comfort of your home.
Comparison Table: Treatment Approaches
| Feature | PCOS Hair Loss | Menopause Hair Loss |
|---|---|---|
| Primary Medical Treatments | Spironolactone, Metformin, Oral Contraceptives | Hormone Replacement Therapy (HRT), Estrogens |
| Topical Options | Minoxidil 2% or 5% | Minoxidil 2% or 5% |
| Treatment Goal | Reduce androgens, manage insulin resistance | Restore estrogen levels, support hair follicles |
| Lifestyle Focus | Weight loss, low-glycemic diet, regular exercise | Stress reduction, nutrient-rich diet, scalp care |
| Expected Timeline | Results in 3–6 months; full recovery in 9–12 months | Requires ongoing management |
| Telehealth Solutions | Hormone coaching, androgen-blocking prescriptions | Custom HRT plans, dermatologist support |
sbb-itb-6dba428
Why Female Hair Loss Is So Tricky 👩⚕️🧬
Conclusion
Hair loss linked to PCOS stems from excess androgens and insulin resistance, often showing up as thinning around the crown and frontal hairline. On the other hand, menopausal hair loss is caused by declining estrogen levels, leading to more widespread thinning across the top and sides of the scalp in midlife. These differences in causes highlight the need for treatments tailored to the specific hormonal changes behind each condition.
For PCOS, treatments work best when focused on reducing androgens and improving insulin sensitivity. For menopause, addressing estrogen deficiency is key. In both cases, topical or oral Minoxidil can help, but tackling the root hormonal imbalance is essential for long-term results.
Managing hormonal hair loss requires expertise across multiple fields, including endocrinology, dermatology, and gynecology. With the right knowledge, women can choose treatments that suit their unique hormonal needs. Services like Oana Health make this process easier by connecting individuals with licensed professionals who can prescribe targeted therapies and deliver them straight to your home.
Whether you're dealing with hair loss from PCOS or menopause, identifying the root cause is the first step toward effective treatment. Acting early increases the chances of slowing hair loss and encouraging regrowth, making timely and specialized care crucial for maintaining hair health.
FAQs
What causes hair loss in PCOS compared to menopause?
The reasons behind hair loss in PCOS and menopause stem from very different hormonal changes.
For those with PCOS, the main culprits are elevated androgens, like testosterone and dihydrotestosterone (DHT). These hormones interfere with the hair growth cycle, making it shorter, and cause hair follicles to shrink. This often leads to thinning hair, particularly at the crown or along the part line.
In menopause, the story is different. Hair loss here is linked to a steep decline in estrogen and progesterone levels. This hormonal shift disrupts the balance with androgens, reducing estrogen's protective role on hair follicles. As a result, thinning hair often becomes noticeable after menopause.
To sum it up, PCOS-related hair loss stems from an excess of androgens, while menopause-related hair loss is due to a drop in estrogen and progesterone, which leaves the effects of androgens more pronounced.
How can lifestyle changes help manage PCOS-related hair loss alongside medical treatments?
Lifestyle adjustments can work hand-in-hand with medical treatments to tackle PCOS-related hair loss by addressing the hormonal imbalances driving the issue. Even shedding just 5% of body weight can help lower testosterone levels and improve insulin sensitivity, which in turn reduces the hormonal triggers behind hair thinning. Pairing a nutrient-dense diet - one lower in dairy and carbohydrates - with regular aerobic and resistance exercises can further enhance these hormonal shifts while boosting blood flow to the hair follicles.
Stress management also plays a key role. Practices like mindfulness, yoga, or simply ensuring you get enough sleep can help protect your hair follicles from additional strain. On top of that, making sure your diet includes essential nutrients like iron, zinc, vitamin D, and biotin can support healthy hair growth. When these lifestyle habits are combined with medical treatments, such as anti-androgens or topical solutions, women with PCOS often see more noticeable and lasting improvements in their hair health. Oana Health offers personalized telehealth programs designed to blend these lifestyle strategies with tailored medical care, helping women achieve better outcomes and long-term success.
Can hair loss during menopause be reversed, or is it usually permanent?
Hair loss during menopause can often be managed and, in some cases, reversed with the right care. Many women find relief through hormonal therapies, topical treatments, or adjustments to their lifestyle that align with their individual needs. The success of these treatments largely depends on factors like the root cause of the hair loss and how quickly it's addressed.
If menopausal hair loss is affecting you, reaching out to a healthcare provider can help pinpoint the most effective solutions. Taking action early can boost the chances of seeing improvements and encourage healthier hair growth over time.